


Read more about the author Dr Shreya Armstrong
Epidemiology
Skin cancer accounts for the largest number of cancers diagnosed in Australia each year, with more non melanoma skin cancer (NMSC) diagnosed each year than all cancers combined1. The common NMSCs include basal cell carcinoma (BCC) and squamous cell carcinoma (SCC), with 35% increase in age standardized incidence of BCC and double the incidence of SCC from 1985 to 2002. Rarer NMSCs include but are not limited to Merkel cell carcinoma and dermatofibrosarcoma, with 900 new cases diagnosed in Australia in 2016, accounting for 0.7% of all cancers diagnosed. Australia also has the world’s second highest incidence of melanoma, with 35 new cases a year per 100,000 people, accounting for 10% of all cancers diagnosed1.
Treatment Options for Skin Cancer
The treatment options available for skin cancer includes topical therapies, surgery, radiation therapy, systemic therapy (including chemotherapy, immunotherapy and/or targeted therapy), either alone or in combination. The ultimate choice of treatment depends on the tumour type, tumour extent, patient fitness and patient preference.
Radiotherapy for Skin Cancer
For NMSCs, radiotherapy can be used as the sole definitive treatment modality, or in the adjuvant setting for tumours with high risk features to reduce the risk of local recurrence (see table below). Definitive radiotherapy may be considered for patients who are not a surgical candidate, present with an inoperable lesion, or where excision would produce loss of function or unacceptable cosmesis. Randomised data comparing different treatment modalities are lacking, however large series data report local control rates with radiotherapy in the order of 90-95% and excellent or good cosmesis in >90% of patients3-7. Merkel cell carcinomas (MCCs) are aggressive neuroendocrine tumours with high propensity for regional and distant metastases. MCCs are exquisitely radiosensitive, with two meta-analyses confirming the benefit of adjuvant radiotherapy, which is associated with significant improvement in locoregional control and overall survival compared to surgery alone. MCC may also be managed with definitive radiotherapy alone, with reported in-field control rate of 75%8.
For melanoma, adjuvant radiotherapy may be considered for patients at high risk of local or regional recurrence. Randomised evidence has shown the addition of adjuvant radiotherapy for tumours with high risk features is associated with a statistically significant reduction in locoregional relapse9.
|
Indications for post-operative radiotherapy for NMSCs (adapted from eviQ)2 |
|
Absolute - T4 disease - Positive margins, where further surgery not feasible - Large nerve perineural spread - Recurrent disease |
|
Relative (consider when 2 or more present) - T2 or T3 - Poorly differentiated - Close margins (<2mm) - ≥6mm depth of invasion - Lymphovascular invasion - Immunosuppression - Pathological perineural invasion (nerve diameter ≥0.1mm) - High risk tumour site (e.g. preauricular, ear, temple, non-hair bearing lip) |
Management of Skin Cancer at North Coast Cancer Institute (NCCI)
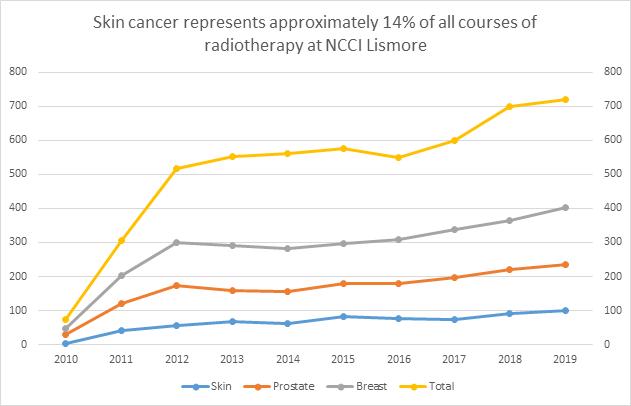
At NCCI, skin cancer is the 4th most common tumour type treated.
The location, size, depth and overall volume of the tumour dictates which modality of radiotherapy is most suitable. According to the clinical parameters, patients at NCCI may be treated using superficial radiation therapy (SXRT) or external beam radiotherapy (EBRT).
SXRT is used to treat small tumours in eloquent and/or technically challenging locations such as lesions near the eye or nose. Majority of skin cancers are treated using EBRT, including superficial tumours that are not suited for SXRT and for tumours where larger and more complex volumes require treatment.
Technological advances in radiotherapy mean that complex surfaces such as scalp or regional lymph nodes can be treated at NCCI using modern EBRT techniques such as intensity modulated radiation therapy (IMRT) or volumetric modulated arc therapy (VMAT). These techniques allow for a sophisticated delivery whereby the high doses of radiation can be delivered to clinical regions at risk whilst minimizing unnecessary side effects.
Radiotherapy dose to healthy tissues
Radiotherapy referrals to NCCI are received either directly (via general practitioners, surgeons or dermatologists), or more complex cases are discussed and referred through a multidisciplinary team meeting (MDT) pathway. Our local MDM is held fortnightly, and typically attended by surgeons, radiation oncologists, medical oncologists, pathologists and radiologists. We welcome the involvement of general practitioners at the meeting, which can attend either physically or virtually at Lismore Base Hospital.

The figure above illustrates a series of clinical photographs of a patient with multiple NMSCs prior to radiotherapy in the top row, followed by a series of clinical photographs following a course of definitive radiotherapy (using SXT), showing complete clinical response.
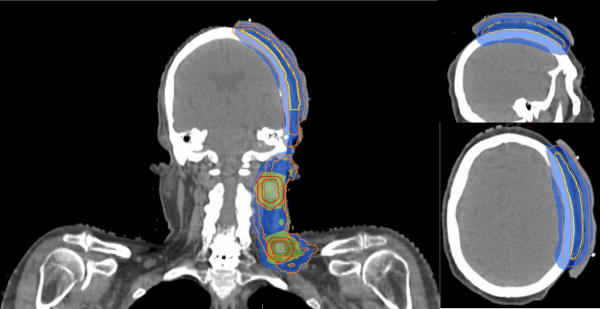
This figure illustrates a complex radiotherapy plan using VMAT technique for patient with high risk cutaneous SCC with pathological lymph nodes in the left neck. The blue and green highlighted areas represent the differential dose prescription to the overall volume, with a higher radiation dose prescribed to the pathological macroscopic neck nodes.
References
- Australian Institute of health and Welfare 2016. Skin Cancer in Australia: An overview, 2016. AIHW, Cat no CAN 96 Canberra 2016.
- EviQ. Skin cancer squamous cell carcinoma adjuvant EBRT post-operative, ID 1033 version 3. EviQ, NSW 2020.
- Veness, M.J. 2008. The important role of radiotherapy in patients with non-melanoma skin cancer and other cutaneous entities. J Med Imaging Radiat Oncol 52(3):278-286.
- Locke, J., S. Karimpour, G. Young, et al. 2001. Radiotherapy for epithelial skin cancer. Int J Radiat Oncol Biol Phys 51(3):748-755.
- Silverman, M.K., A.W. Kopf, A.H. Gladstein et al. 1992. Recurrence rates of treated basal cell carcinomas. Part 4: X-ray therapy. J Dermatol Surg Oncol 18(7):549-554.
- Cognetta, A.B., B.M. Howard, H.P. Heaton, et al. 2012. Superficial x-ray in the treatment of basal and squamous cell carcinomas: a viable option in select patients. J Am Acad Dermatol 67(6):1235-1241. 7. Pampena, R., T. Palmieri, A. Kyrgidis, et al. 2016. Orthovoltage radiotherapy for nonmelanoma skin cancer (NMSC): Comparison between 2 different schedules. J Am Acad Dermatol 74(2):341-347. 8. Veness M., M. Foote, V. Gebski, et al. 2010. The role of radiotherapy alone in patients with merkel cell carcinoma: reporting the Australian experience of 43 patients. Int J Radiat Oncol Biol Phys 78(3):701- 709.
- Burmeister, B. H., B. Mark Smithers, E. Burmeister, et al. 2006. A prospective phase II study of adjuvant postoperative radiation therapy following nodal surgery in malignant melanoma- Trans Tasman Radiation Oncology Group (TROG) Study 96.06. Radiother Oncol 81(2):136-142.
About the author - Dr Shreya Armstrong
 Dr Shreya Armstrong has joined Drs Patrick Dwyer, Julan Amalaseelan and A/Prof Tom Shakespeare at the North Coast Cancer Institute.
Dr Shreya Armstrong has joined Drs Patrick Dwyer, Julan Amalaseelan and A/Prof Tom Shakespeare at the North Coast Cancer Institute.
Shreya completed her specialist training in Radiation Oncology in 2014, having undertaken the first two years of training in New South Wales at Newcastle Calvary Mater Hospital and Lismore Base Hospital, before going on to Royal Brisbane and Women’s Hospital and Princess Alexandra Hospital. She subsequently undertook the Windeyer Fellowship at Mount Vernon Hospital in the United Kingdom specialising in brachytherapy for urological and gynaecological malignancies.
She has had several papers published and has presented at clinical research conferences both nationally and internationally.
Shreya has a special interest in cutaneous, central nervous system, gynaecological and urological malignancies, as well as palliative radiotherapy for all tumour sites.
She consults at the outpatient clinic at Lismore Base and at the soon to be established radiation outpatient clinic at Byron Central Hospital.
Shreya returned to the beautiful North Coast having been impressed by the area and its community when she first came as a registrar.
She can be contacted through the NCCI or at











